|
|
Mitral Stenosis
- Rheumatic disease causes mitral stenosis in 99.8% of cases
- Acute rheumatic fever (ARF) → pancarditis
- Mitral valve most commonly involved valve
- Followed by mitral and aortic together
- Then by aortic alone
- Acute phase → cardiomegaly
- Mitral regurgitation is valvular lesion of ARF
- As acute phase subsides, fibrosis alters leaflet or cusp structure
- Results in cuspal or leaflet thickening along valvular margins of closure
- Mitral Valve Calcification
- Calcium usually deposited in clumps on valve leaflets
- Heavier calcific deposits in men than women
- Calcification of mitral annulus does not signify presence of mitral valve disease
- Mitral orifice becomes smaller → two circulatory changes
- To maintain LV filling across narrowed valve, left atrial pressure goes up
- Blood flow across mitral valve is decreased which decreases cardiac output
- Mitral Valve Areas
- Normal mitral valve orifice 4-6 sq cm in adults
- When reduced to <2 sq cm, LA pressure increases
- Gradient across mitral valve is hallmark of mitral stenosis
- About 20 mm Hg in mitral stenosis
- MS and MR
- Rheumatic mitral stenosis occurs with varying degrees of mitral regurgitation
- When MS is severe, MR is relatively unimportant
- Effect of MS on Heart
- Left atrium hypertrophies and dilates 2° pressure and volume load
- Atrial fibrillation and mural thrombosis follow
- Left ventricle is “protected” by stenotic valve
- Usually normal in size and contour
- Effect of MS on Lungs
- Increased pulmonary venous and capillary pressure
- Chronic edema of alveolar walls → fibrosis
- Pulmonary hemosiderin is deposited in lungs
- Pulmonary ossification may occur
- Effect of MS on Lungs
- Pulmonary arterial hypertension develops
- First passively
- Then 2° muscular hypertrophy and hyperplasia → increased pulmonary vascular resistance
- Effect of MS on Right Ventricle
- RV hypertrophies in response to increased afterload
- Eventually RV fails and dilates
- Causes dilation of tricuspid annulus → tricuspid regurgitation
Mitral Stenosis-Other Causes
- Congenital Mitral Stenosis
- Exists as isolated abnormality 25% of time
- Coexists with VSD 30% of time
- Coexists with another form of left ventricular outflow obstruction 40% of time—SHONE’S Syndrome
- Shone’s Syndrome
- Parachute mitral valve
- Supravalvular mitral ring
- Subaortic stenosis
- Coarctation of aorta
- Infective Endocarditis
- Large vegetations occurring on previously normal mitral valve may produce MS
- Carcinoid Syndrome
- Carcinoid of lung allows for prolonged exposure of mitral valve to serotonin
- May result in stiff, stenotic mitral valve
- Fabry’s Disease
- Deposition of aramide trihexoside thickens and decreases mobility of mitral leaflets
- Hurler’s Syndrome
- Deposition of mucopolysaccharide thickens and decreases mobility of mitral leaflets
- Whipple’s Disease
- Same as gut lesions in mitral leaflets
- LA Myxoma
- Most common form of primary cardiac tumor
- 86% of myxomas are found in left atrium
- 90% of myxomas are solitary
- Usually occur around fossa ovalis
Imaging Findings of MS
- Cardiac Findings
- Usually normal or slightly enlarged cardio-thoracic ratio
- Straightening of left heart border
- Convexity of left heart border 2° to enlarged atrial appendage--only in rheumatic heart disease
- Small aortic knob from decreased cardiac output
- Double density of left atrial enlargement
- Rarely, right atrial enlargement from tricuspid insufficiency
- MS-Calcifications
- Calcification of mitral valve--not annulus--seen best on lateral film at fluoroscopy
- Rarely, calcification of the left atrial wall 2° fibrosis from long-standing disease
- Rarely, calcification of pulmonary arteries from PAH
- MS-Pulmonary Findings
- Cephalization
- Elevation of left mainstem bronchus (especially if 90° to trachea)
- With severe, chronic disease enlargement of the main pulmonary artery from pulmonary arterial hypertension
- Mitral Stenosis-Echocardiographic Findings
- In 90%, M-mode study will demonstrate flattening of E-F slope
- Decreased diastolic excursions of mitral leaflets
- Concordant anterior movement of anterior and posterior leaflets during systole
- Mitral Stenosis-Echocardiographic Findings
- If left atrium > 5cm, increased incidence of
- Atrial fibrillation
- Left atrial thrombus
- Systemic embolization
- Mitral Stenosis-Angiographic Findings
- Ventriculography in 30 to 40° RAO projection usually used
- Severity of lesion determined hemodynamically by simultaneously measuring Pulmonary capillary wedge pressure, Left ventricular inflow tract pressure and Cardiac output
- Mitral Stenosis-Angiographic Findings
- Calcified, hypokinetic and domed mitral leaflets
- Enlargement of left atrium
- Left ventricle is small with a reduced ejection fraction
- Mitral valve leaflets appear thickened and nodular and may appear to attach directly to the papillary muscle
- Scarring and retraction of the chorda tendina
 
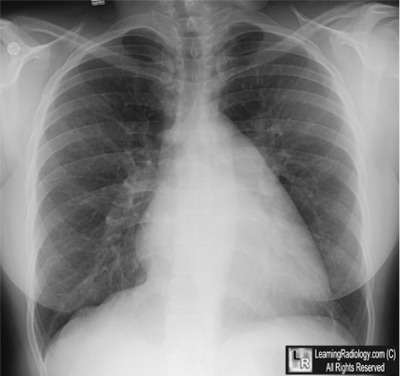
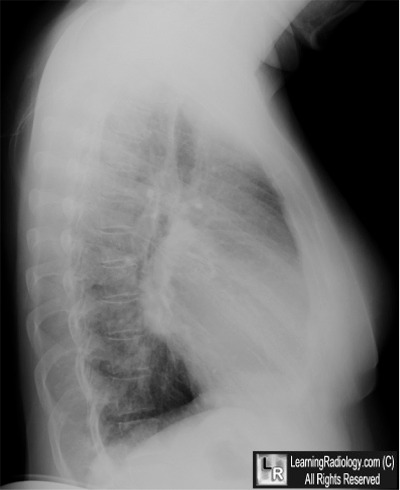
Mitral Stenosis. The frontal chest radiograph demonstrates an enlarged left atrium (white arrow) which is also seen to be elevating the left main bronchus (blue arrow). The blood vessels at the apex are at least as large as those at the base in this upright chest indicating cephalization and elevated pulmonary venous pressure (white circle). The lateral chest radiograph shows an enlarged left atrium bulging posteriorly in the middle of the cardiac shadow (blue arrow).
For these same photos without the arrows, click here and here
For more information, click on the link if you see this icon 
|
|
|

{kind=link}
{kind=link}